Original Article
Year: 2022 |Volume: 3 | Issue: 01 |Pages: 65-72
Comparative study of Dahan karma and Conjunctivo-limbal autograft Chikitsa in the management of “Arma” (Pterygium).
About Author
Correspondence Address:
Dr. Manisha Dehankar( Gotmare) Associate Professor, Dept of Shalakyatantra,DMAMC, Wanadongari. Hingna Nagpur.
Date of Acceptance: 2022-01-19
Date of Publication:2022-02-10
Article-ID:IJIM_139_02_22 http://ijim.co.in
Source of Support: nil
Conflict of Interest: nil
How To Cite This Article: Dehankar M, Bagde S,Dakhore J.R. Comparative study of Dahan karma and Conjunctivo-limbal autograft chikitsa in the management of “Arma” (Pterygium). Int J Ind Med 2022;3(1):65-72
Abstract
“Arma” is one of the shuklamandalgat disease and is described as the continuous outgrowth in shuklamandal. “Arma” is triangular fibrovascular growth encroaching on cornea (krishnamandal and drishtimandal) from inner and outer canthus of eye. Objectives:Comparative study of Dahan karma and Conjunctivo-limbal autograft chikitsa in the management of “Arma” (Pterygium). To study the recurrence rates of “Arma” after Dahan karma and conjunctivo-limbal autograft treatments. Materials and Methods: This is a prospective, randomized, interventional, hospital based, comparative study. Study period-All the surgeries were performed from August 2009 to June 2010 with primary, progressive pterygium were included in experimental group (Group A) and 30 patients in control group (Group B) respectively. Conclusion: Bare sclera with CLAU is a better technique to prevent recurrence of Pterygium. Both techniques are equally safe. Bare sclera with CLAU can be established as line of treatment of Arma to prevent its recurrence after surgical excision.
Keywords: Arma, shuklamandal, Arma, pterygium, Chhedya vyadhi
Introduction
Ayurveda is an ancient science which deals with healthy wellbeing of person and treatment of diseased one. It has a noble aim of healthy body and healthy mind of each and every individual. As India is a topical country, due to hot, sandy, dry climate and outdoor occupations, maximum and continuous exposure to UV rays, dark skin complexion and genetic predisposition leads to various systemic and especially ocular diseases like “Pterygium ”.1 Arma” is one of the shuklamandalgat disease and is described as the continuous outgrowth in shuklamandal.2 On the basis of signs and symptoms described by modern medical science, the disease “Arma” can be compared with “Pterygium” in modern ophthalmology. It is an elastoid degeneration of subconjunctival tissue which proliferates as vascularised granulation tissue to invade the cornea, destroying Bowman’s membrane and superficial stroma, the whole being covered with conjunctival epithelium.3 According to Sushrutacharya “Arma” comes under Shuklagat rogas of eye and among 11 Shuklagat rogas Armas are 5 in number.4 “Arma” is triangular fibrovascular growth encroaching on cornea (krishnamandal and drishtimandal) from inner and outer canthus of eye. According to Acharya Sushrut “Arma” is Chhedya vyadhi but if it is asymptomatic then it is left untreated.5 The “Arma” is treated only if it shows symptoms. Usually, it is treated for progression towards pupillary area, excessive astigmatism, poor cosmesis.6 But recurrence rate is more after excision of Arma. The study has been done to find out and to compare the minimal recurrence rate amongst these two procedures and to give the permanent and safe root of treatment in the management of Arma.
Objectives:
-
To study the details of “Arma” disease described in Shuklagat diseases of eye according to Ayurveda and Modern Sciences.
-
Comparative study of Dahan karma and Conjunctivo-limbal autograft chikitsa in the management of “Arma” (Pterygium).
-
To study the recurrance rates of “Arma” after Dahan karma and conjunctivo-limbal autograft treatments.
Materials and Methods-
This is a prospective, randomized, interventional, hospital based, comparative study.
Study period-All the surgeries were performed from August 2009 to June 2010.
Total 60 eyes of 60 patients who came to our institute (Govt. Ayurved Hospital) with primary, progressive pterygium were included in experimental group (Group A) and 30 patients in control group (Group B) respectively.
Inclusion Criterion -
-
The patients who came to OPD of Shalakya Tantra in our hospital and were diagnosed of having primary, progressive pterygium.
-
Patients who were in the age group of 20 to 70 years were selected randomly.
-
The patients who met the indications of surgical treatment.
-
The patients who signed the informed consent to enrol into the study i.e. Patients who are ready to accept our treatment.
Exclusion Criteria-
-
Patients suffering from type 1 Arma.
-
The patient suffering from any active ocular disease like conjunctivitis, corneal ulcer, iridocyclitis were rejected.
-
The patients who had recurrent pterygium.
-
Patients who refused to accept our treatment.
Clinical Evaluation-
-
In experimental group(Group A)30 patients were undergone, pterygium excision with conjunctivo-limbal autograft.
-
In active control group (Group B), 30 patients were undergone pterygium excision with Dahan karma.
-
Patients of exclusion criterion were not taken in study.
Criteria for evaluation (parameters)-
1. Grade 0 – Absent or no growth
2. Grade 1 – Extend less than 2 mm onto the cornea. It is asymptomatic.
3. Grade 2 – Extend up to 4 mm of cornea, may be primary or recurrent following surgery.
4. Grade 3 – Invade more than 4 mm of cornea and involving the visual axis.
Pre-operative medication-
1. Topical Antibiotics-
a) Ofloxacine eye drop QID for 3 days just before surgery is advisable as prophylaxis.
b) Flurbiprofen eye drop, should be instilled three times one day before surgery and haif hourly for two hours immediately before surgery.
2. Inj.Titanus toxoid given intramuscularly.
3. Inj.Xylocain 2% S/C given for testing sensitivity.
4. Preparation of eye to be operated-
Eyelashes of upper lid should be trimmed at night and the eye to be operated should be marked. An informed and detailed consent should be obtained.
Anaesthesia- All patients were operated under peribulbar block using 2 % xylocaine + 1:2,00,000 adrenaline 3 cc and 0.5% bupivacaine 2 cc with inj.hylurunidase 5IU/ml.
Follow ups-
All patients were followed up at 24 hours, 3rd day, 1st week, 15th day, 1month, 2nd month, 4th month and 6th month post-operatively.
tables
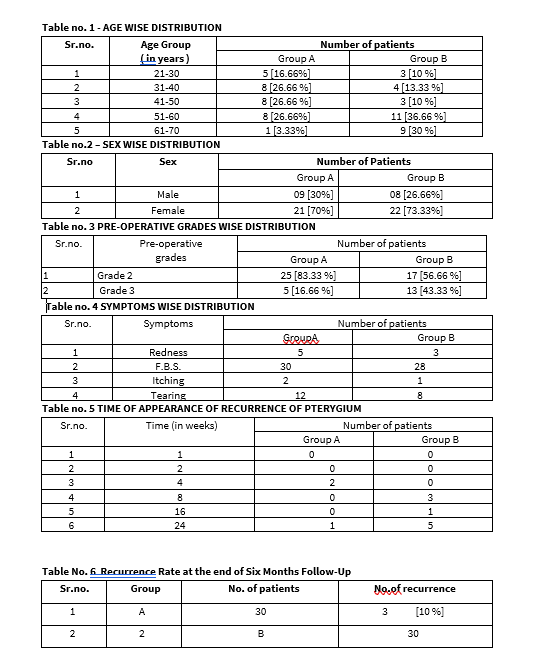
Table no. 1 shows age-wise distribution of study patients. In the age group of 21-30 years 5 patients (16.66%) were from Group A and 3 patients (10 %) were from Group B. In the age group of 31-40 years 8 patients (26.66 %) were from Group A and 4 patients (13.33 %) were from Group B. In the age group of 41-50 years 8 patients (26.66 %) were from Group A and 3 patients (10%) were from Group B. In the age group of 51-60 years 8 patients (26.66 %) were from Group A and 11 patients (36.66 %) were from Group B.In the age group 61-70 years 1(3.33%) patient was from group A and 9 patients were from group B (30%).
Table no. 2 shows sex-wise distribution of study patients. Out of 60 patients in the study 9 patients (30 %) from Group A were males and 21 patients (70 %) were females. 8 patients (26.66 %) from Group B were males and 22 patients (73.33 %) were females.
Table no. 3 shows pre-operative grades wise distribution of pterygium in study patients. In Group A, 25 patients (83.33 %) were having Grade 2 pterygium, 5 patients (16.66 %) were having Grade 3 pterygium. In Group B, 17 patients (56.66 %) were having Grade 2 pterygium, 13 patients (43.33 %) were having Grade 3 pterygium.
Table no. 4 shows symptoms wise distribution in study patients. In Group A, 5 patients were having redness, 30 patients were having foreign body sensation, 2 patients were having itching, 12 patient was having tearing. In Group B, 3 patients were having redness, 28 patients were having foreign body sensation, 1 patient was having itching, 8 patients were having tearing.
Table no. 5 shows time of appearance of recurrence of Pterygium in study patients. In Group A, there was recurrence in 2 patients in 4th week and 1 patient was having recurrence in 24th week. In Group B, there was recurrence in 3 patients in 8th week, 1 patient was having recurrence in 16th week, 5 patients in 24th week.
Table no. 6 Shows recurrence rate of pterygium in study patients after six months follow-up. In Group A, there was recurrence in 3 patients (10 %) out of 30 patients. In Group B, there was recurrence in 9 patients (30 %) out of 30 patients.
Comparative result of group A and group B in preventing recurrence of pterygium after its surgical excision.As it is a qualitative data so to evaluate the role of Agnikarma in preventing recurrence of pterygium compared to bare sclera technique ‘Z’ test was applied. Value of Z is more than 1.96. The critical level of significance since it is significant at 95% of confidence limit.
Discussion
Pterygium is characterized by excessive fibro-vascular proliferation on the exposed ocular surface and is thought to be caused by increased UV radiation exposure, from climatic factors and aggravated by microtrauma and chronic inflammation from environmental factors.7 Despite the multi- factorial pathogenesis, surgery is the main treatment. The primary concern of the pterygium surgery is recurrence i.e. re-growth of the fibro-vascular tissue across the limbus and onto the cornea. It is believed that surgical trauma and subsequent post-operative inflammation may be a cause of pterygium recurrence.8
In the present study the youngest patient was 25 years old and the oldest was 66 years old. Average age of the study patients was 45+_5 years. 8 out of 60 patients (13.33 %) were in the age group of 20-30 years. 12 out of 60 patients (20 %) were in the age group of 30-40 years. 11 out of 60 patients (18.33%) were in the age group of 40-50 years. And 19 out of 60 patients (31.66 %) were in the age group of 50- 60 years.10 out of 60 patients (16.66)were in the age group of 61-70 years. This shows that there exists a positive relationship between pterygium and age of the patient. The patients who came to our institute were lacking in health status awareness, especially for geriatric population. Many of the old age group patients did not consider pterygium as the disease requiring treatment and hence were not willing for surgery. The awareness regarding pterygium and willingness to undergo surgery for the same was more in younger age group patients. This could have led to the results found in the present study. The age-group wise distribution found in present study cannot be the representative of age-wise distribution of pterygium either in patients presenting in Shalakya OPD of our institute or population in general.
In the present study 17 out of 60 patients (28.33 %) were males and 43 out of 60 patients (71.66 %) were females. This shows that females outnumbered the males. In this study 36 patients out of 60 (60 %) were pursuing outdoor occupation and 24 out of 60 (40 %) were pursuing indoor occupation in the present study. Outdoor occupation is a known risk factor for development of pterygium. The probable reason of this is increased exposure to heat, dust and dry environment. In our country increased outdoor activity means increased exposure to sunlight and UV radiations. According to theory UV radiation causes p 53 gene mutagenesis in pterygium fibroblasts leading to uncontrolled cellular proliferations. This could be the most important reason for higher proportion of patients being outdoor workers in present study.
Majority of pterygia in the study were nasal i.e. 88.33% and 9.99 % of pterygia were bilateral. A temporal pterygium without a nasal was not found in the study. This shows that pterygium is more common on nasal side than temporal side. In the present study 19 out of 60 patients (31.66 %) had pterygium only in right eye, and 16 out of 60 patients (26.66 %) had pterygium only in left eye and remaing 25 out of 60 patients (41.66 %) had bilateral pterygia.
Out of the two surgical techniques under study none had serious vision threatening complications. All patients had conjunctival congestion post-operatively due to surgical trauma and which cleared with topical steroid and antibiotic eye-drops and systemic anti-inflammatory therapy.
Conclusion
This is a prospective, interventional, hospital based, comparative study in which 60 eyes of 60 patients with primary progressive Pterygium were included in study. Two groups of 30 patients each, underwent Pterygium excision with CLAUtechnique and plain bare sclera with Dahan karma technique. The main outcome measurement was recurrence rate after surgery. Fleshiness of Pterygium was found to be a risk factor for recurrence after surgery. Duration of appearance of recurrence after surgery was 4 weeks or more. Bare sclera excision + dahankarma technique had higher recurrence rate than bare sclera + CLAU technique. Although bare sclera+dahankarma technique is a technically much easier procedure, its high recurrence rate makes its recommendations as a primary modality for surgical treatment of Pterygium very difficult. Bare sclera with CLAU is a better technique to prevent recurrence of Pterygium. Both techniques are equally safe. Bare sclera with CLAU can be established as line of treatment of Arma to prevent its recurrence after surgical excision.
References
- Jack J Kanski: clinical ophthalmology, conjunctiva, Butterworth Helmann Elsevier: 6th Edition : Reprint 2008 : pg no. 242, 243, 245.
- Dr. Ambikadatta Sastri : Susruta Samhita Uttaratantra 15/17; Chaukhambha publications, Varanasi; Edition-Reprint : 2006; pg no.53
- A K Khurana & Aruj K Khurana. Comprehensive Ophthalmology. New Delhi. Jaypee Brothers Medical Publishers (P) Ltd. 6, 623, 59.
- Dr. Ambikadatta Sastri : Susruta Samhita Uttaratantra 15/19; Chaukhambha publications, Varanasi; Edition-Reprint : 2006; pg no.53
- Sushrutha Samhita, with Sri Dalhanacharya teeka, edited by Narayan Ram Acharya “Kavyathirtha”, Chaukhambha orientalia, Varanasi, reprint edition-2009, Uttaratantra, 18(6), 824,596
- Astanga Sangrah vriddha vagbhata with the Shashilekha Sanskrit commentary by Indu, edited by Dr.Shivprasad Sharma,Uttartantra vol 3; 14/16; Chaukhambha publications, Varanasi; Edition-Reprint : 2006;pg no.124
- Ramanjit Sihota & Radhika Tandon. Parsons? Diseases of the Eye. New Delhi. Elsevier- A division of Reed Elsevier India Pvt. Ltd. 21, 2011. 184.
- A K Khurana & Aruj K Khurana. Comprehensive Ophthalmology. New Delhi. Jaypee Brothers Medical Publishers (P) Ltd. 6, 623, 88
